Hope
this season is filled with Lots of happiness and joy, wealth and prosperity.
May your home be filled with love on this wonderful occasion of Thanksgiving!

Cohesive Journal of Microbiology & Infectious Disease_Crimson Publishers
Hope
this season is filled with Lots of happiness and joy, wealth and prosperity.
May your home be filled with love on this wonderful occasion of Thanksgiving!
Comparison of Ultrabio HIV DNA PCR and Gag Real-Time PCR Assays for Total Hiv-1 DNA Quantification by Tuofu Zhu in Cohesive Journal of Microbiology & Infectious Disease
https://crimsonpublishers.com/cjmi/fulltext/CJMI.000572.php

Background: AIDs is still the leading cause of death in the global community more especially in Sub-Sahara Africa including Eswatini. To fast track uptake of Antiretroviral therapy in Eswatini Test and Start has been introduced, aimed at initiating all people living with HIV on ART as soon as possible after diagnosis regardless of CD4 count, viral load or clinical stage. Knowledge and attitude of nurses towards the Test and Start program is an important consideration in improving ART uptake. Hence the study aimed at investigating the knowledge and attitudes of nurses on Test and Start in one referral hospital in Eswatini.
Methods: A descriptive, cross-sectional quantitative design was employed among 50 participants, selected through simple random sampling. All participants were registered nurses with at-least one-year work experience in departments providing Test and Start. An adapted, self-administered questionnaire was used to collect data. Data was analyzed using descriptive statistics and Pearson’s correlation.
Findings: All participants (100%, N=50) reported to have heard about Test and Start, 50% (n = 25) obtained information from integrated trainings (which were basically for other courses and only 2% from literature. Most of them (56%, n=28) have not been formally educated, but they all knew the definition of Test and Start, only 12% (n=6) did not know the eligibility criteria for Test and Start. About 56% (n=28) complained that its increased workload, 62% (n=31) complained that Test and Start is complicated. There was a statistically significant association between knowledge and attitudes on Test and Start (r =0.394, p=0.005). Training was also significantly related with attitudes on Test and Start (r=0.349, p=0.013)
Conclusion: Awareness was high but there was knowledge deficit among nurses on Test and Start. Few nurses were trained on Test and Start hence the attitudes were reported negative towards the initiative.
Keywords: Knowledge; Attitudes; Test & Start; HIV; Antiretroviral therapy
Human Immune Deficiency Virus (HIV) and Acquired Immuno-Deficiency Syndrome (AIDS) are a Public Health concern because the number of cases has increased dramatically over the last ten years (World Health Organization [WHO], 2015). Therefore, it is imperative that health care workers possess appropriate knowledge and attitudes towards HIV management in order to ensure quality HIV care to patients. Although 90% of people newly infected with HIV live in just 35 countries, the HIV epidemic remains global, affecting every part of the world and adding substantially to health burdens in many regions UNAIDS. Epidemic patterns, progress and challenges however vary considerably. The AIDS epidemic continues to disproportionately affect sub-Saharan Africa, which is home to 26 million people living with HIV. In 2014, there was an estimated 1.4 million new HIV infections, approximately 66% of the global total UNAIDS. In Swaziland 222 000 people are estimated to be living with HIV. This has become an awakening call to the global health governing body WHO and other agencies to endlessly seek strategies to address the issue. Therefore, international community has committed to ending the AIDS epidemic as a public health threat by 2030, which is a target of the 2030 Agenda for Sustainable Development Goals adopted by the United Nations General Assembly in September 2015 (WHO, 2015). On another note, interim targets have been established for 2020, coined the “90-90-90”. As of consequence the first 90 states that by 2020 90% of all people living with HIV will know their HIV status, the second 90 suggests that 90% of all people diagnosed with HIV will receive sustained antiretroviral therapy (ART) and the last 90 suggests that 90% of all people receiving ART will be virally suppressed. This is a global benchmark target aiming to end AIDS. As a result, WHO (2015) came up with a recommendation of fast tracking these targets by introducing Test and Start initiative [1-8].
The Test and Start program are a strategy that aims to initiate all people living with HIV on antiretroviral therapy (ART) as soon as possible after diagnosis of HIV infection, irrespective of CD4 count, viral load or clinical stage (MoH, 2015). The benefits of Test and Start however are undeniable. If individuals know their status and initiated ART early are likely to contribute to reduction of morbidity and mortality related to HIV (MoH 2016). The Temprano study showed 44% reduction in morbidity with ART at CD4 above 500 cells/mm3 than the standard practice. Other benefits are preventing lost to follow-up clients enrolled on PreART after a positive test result, as most of them are initiated same day rather than appointing another day. Nurses who are not knowledgeable on such benefits may not be able to market this product effectively as they will be not sure if it really works and what to say when the client require explanations on some issues on Test and Start, as a result they will not implement the initiative. A review by The Joint United Nations Programme on HIV/AIDS [UNAIDS] (2014), states that some countries are making notable progress in scaling up access to treatment. Furthermore, the authors reported that globally the number of people receiving HIV treatment had increased from 2.2 million in 2005 to over 15 million in 2015. However, treatment coverage varies from country to country and the reasons for different levels of coverage relate, among others, to health care system capacity, HIV related stigma and discrimination as well as access to funding and the cost of treatment. In addition, the reason could also be that of knowledge deficit among health workers and their attitudes towards the initiative, in which, its importance is rarely emphasized. MoH (2015) states that while Swaziland has the highest HIV prevalence in the world (28.1% for ages 15-49 years) only 66% of HIV infected individuals are on ART. This as well, could be attributed to the above-mentioned reasons of treatment coverage variations.
Therefore, to examine knowledge and attitudes among health workers on HIV management various studies have been conducted which have almost the same conclusions. Gledović, Rakočević, Mugoša, and Grgurević (2015) reported that health workers had knowledge deficit concerning HIV management. The study reported that knowledge among doctors was 68% while among nurses and other health professionals was 36% Gledović et al. Furthermore, the study reported that 63.9% of the study participants indicated the need for education and 6% refused to provide health services to HIV positive patients. This shows that knowledge has an influence on how nurses and other health professionals would deliver any service. In addition, Gedu & Tshotsho [4] study reported that the level of knowledge of most of the professional nurses was still of concern as only a few were highly knowledgeable. They also state that health professionals, who render services to HIV and AIDS clients, need to be capacitated and have a positive attitude towards the patients [4]. The confidence to provide HIV services to clients is somehow linked with the level of knowledge the nurse possesses. Iwoi et al. [8] in a study which assessed knowledge and attitudes towards care of people living with HIV among nurses and midwives, supports other studies that there is knowledge deficit among nurses on HIV care approaches including the Test and Start initiative. The study findings revealed that among the respondents of the study, 14.5% had acceptable level of knowledge, 82.4% had moderate and 3.1% had low levels of knowledge pertaining HIV care. Knowledge deficit on HIV care services may contribute to low uptake and rollout of Test and Start. Not only did Iwoi et al. [8] focused on knowledge but also have findings on attitude of nurses, stating that even though there knowledge deficit among the nurses, a majority of them (68.7%) had positive attitudes while 31.3% had negative attitudes towards HIV care services test and start inclusive. Good knowledge was the only predictor of positive attitude towards HIV care. Thus, good knowledge is one important aspect in the success for rolling out the Test and Start initiative.
Swaziland adopted the Test and Start strategy in 2016. Like any other program, it came with many changes in the workplace more especially in the routine enrolment of clients to care. These include intensified testing, re-testing, Pre-ART enrolment, adherence counselling and same day ART initiations. The MoH Swaziland National HIV Test and Start Communication Strategy (2016) reported that on October 1, 2016, Swaziland transitioned the current ART guidelines (The Swaziland integrated HIV management guidelines, 2015) to a National Test and Start Approach bringing the national guidelines to be in line with the global recommendations to initiate ART regardless of CD4 cell count. Hence that is the currently used guide for HIV care in the country which among its policies it states; test the right people in the right places with the right strategies; ensure individuals are linked to care and initiate ART and also ensure high quality care that maximizes retention to care and viral suppression (MoH 2016). Despite all the activities necessary in implementing Test and Start, the issue of health workers’ empowerment is lagging, thus the study seeks to examine the knowledge and attitudes of nurses toward Test and Start initiative. In addition, the study is in line with the MoH (2015) National Health Research Agenda number 6.1.2 which focuses on HIV and AIDS; availability, equity and quality of HIV and AIDS support services among people living with HIV which includes testing and starting ART among People Living with HIV. The aim of the study is to investigate the knowledge and the attitudes of nurses towards Test and Start Initiative in one health facility in the Hhohho region.
A descriptive, cross-sectional quantitative design was used in this study because it provided an objective portrayal of knowledge and attitudes of nurses. The study was conducted in one of the health care facilities in the Hhohho region of Eswatini. Among 118 registered nurses (holders of diplomas and degrees) in departments providing Test and Start services, a sample of 50 participants was obtained by simple random sampling Lipsey [9]. To determine the sample size, a study power size of 80%, significance level (alpha) of 5% and an effect size of 0.5were used. A self-administered questionnaire from a tool adapted from HIV and AIDS toolkit (International Planned Parenthood Federation, 2013). The HIV and AIDS toolkit is comprised of three (3) parts; socio-demographic information, training and experience with people living with HIV, HIV/AIDS knowledge, attitudes and practices. Descriptive statistics and Pearson’s Correlation were used to analyse data which was entered into the Statistical Package of Social Sciences version 20.0. Ethical considerations were adhered to ensure that the participants’ rights were not violated. Permission was sought and obtained from the Eswatini National Health Review and Research Board and the health facility management, as well as informed consent from participants.
A total of 50 participants took part in the study. The response rate was 100%. The findings are presented according to the participants socio-demographic characteristics, and then based on the study objectives.
The socio-demographic characteristics of the participants
Age: the age of the participants ranged between 25 to 53 years. A majority (44%, n=22) were aged between 30-34 years, and 26% (n=13) were aged between 25-29 years. Those aged 40 years and above were 16% (n=8) and 14% were aged between 35-39 years. The mean age of the participants was 33.8 years with a standard deviation of 6.2 years.
Sex: The data showed that most (66%, n=33) participants were predominantly female and only 34% (n=17) were males.
Qualification(s) Almost half (48%, n=24) of the participants were Bachelor’s degree holders, 34% (n=17) had post-diploma certificate in midwifery and mental health, 14% (n=7) were General Nursing Diploma holders and only 4% (n=2) had a Master’s degree.
Work duration: A majority (48%, n=24), of the participants had worked between five (5) to nine (9) years, 22% (n=11) between 1-4 years, 14% (n=7) reported that they had worked for 15 years or more and 8% (n=16) had worked between 10-14 years. The work duration ranged between 1 to 29 years, with a mean of 8.4 years and a standard deviation of 5.8 years. Table 1 summarises the socio-demographic characteristics of the study participants.
Research objective 1
To assess the knowledge of nurses on Test and Start in one health facility in the Hhohho region, Eswatini.
Have ever heard about test and start initiative: All (100%, n = 50) the participants reported that they have heard about the Test and Start initiative.
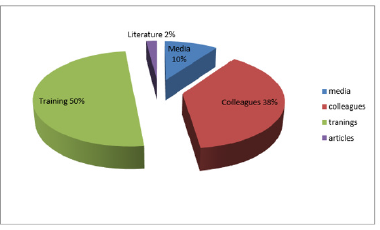
Source of information: Half (50%, n=25) of the participants reported that they got information on the Test and Start initiative from integrated trainings (not merely Test and Start trainings), 38% (n=19) from colleagues, 10% (n=5) from the media and only 2% (n=1) of the participants reported that they obtained information from literature. Sources of information on the Test and Start initiative is graphically summarized in Figures 1 & 2.
Figure 1: Sources of information about test and start initiative (N=50).
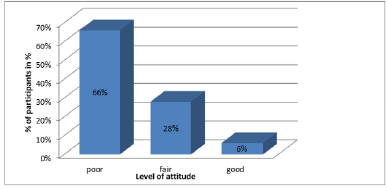
Figure 2: Attitude among the participants towards test and start Initiative (N=50).
Any training on test and start initiative: Most of the participants (56%, n=28) have not been trained on Test and Start and 44% (n=22) of the participants were trained.
Type of training: Among those who were trained, about half (45.5%, n=10) were trained in formal settings, 36.4% (n=8) were trained at work (on the job) and 18.2% (n=4) indicated to have trained both ‘on the job’ and formally.
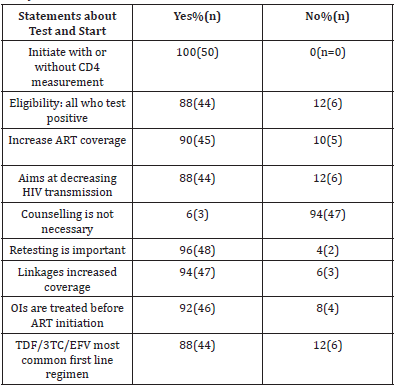
Test and start initiative activities and procedure: All (100%, n = 50) the participants were able to define Test and Start, however, 12% (n=6) did not know the eligibility criteria for Test and Start. A majority (90%, n=45) of participants reported that Test and Start increased ART coverage and only 10% (n=5) reported that Test and Start did not increase ART coverage. On the other hand, 88% (n=44) reported that that Test and Start aimed at decreasing HIV transmission whereas 12%, (n=6), reported that Test and Start did not reduce HIV transmission.
Linkages of other services to test and start: Client linkage to other services improves Test and Start initiative. Most of the participants (94%, n=47) indicated that linkages of HIV services increased ART coverage and only 6% (n=3) reported that linkages don’t increase ART coverage. Knowledge of participants on Test and Start initiative is summarised in Tables 2 & 3.
Table 2: Knowledge of participants on test and start initiative (N = 50).
Table 3:Associations between selected variables (N=50).
IV is the independent variable and DV is the dependant variable.
Adherence counselling: Most of the participants (94%, n=47) indicated that counselling was important under Test and Start and only 6% (n=3) reported that it was not important. Ninety six percent (96%, n=48) of all the participants knew the importance of ‘re-testing for verification’, 4% (n=2) reported that ‘re-testing for verification’ was not important.
Testing for CD4 and test and start: More than half of the participants (64%, n=32) indicated that ART initiation continues with or without CD4 result under Test and Start and 36% (n=18) indicated that no ART initiation without CD4 count.
Treatment of opportunistic infections (OIs) before ART initiation: Eighty four percent (84%, n=42) of the participants indicated that OIs should be treated first before ART initiation to prevent Immune Reconstitution Inflammatory Syndrome (IRIS), and 16% (n=8) indicated that OIs should not treated first.
Commonly used drug combination for first line under test and start: A majority of the participants (88%, n=44) reported that tenofovir disoproxil fumarate/Lamivudine/Efavirenz (TDF/3TC/EFV) was the most commonly used drug combination for first line under Test and Start, and only 12% (n=6) reported it was not.
Participants overall level of knowledge: Above a quarter of the participants (36%, n=18) had good knowledge on Test and Start initiative similarly, 36% (n=18) had moderate knowledge and 28% (n=14) had poor knowledge on Test and Start initiative.
Research objective 2
To determine the attitudes of nurses towards Test and Start in one health facility in the Hhohho region (Eswatini).
Test and Start is an HIV transmission preventive initiative: Most of the participants (76%, n=38) reported that Test and Start was a HIV transmission preventive initiative and only 24% (n=12) reported it was not a preventive initiative.
Test and Start reduces morbidity and mortality: Ninety six percent (96%, n=48) participants also reported that Test and Start was aimed at reducing morbidity and mortality related to HIV and AIDS, and only 4% (n=2) reported that Test and Start was not aimed at reducing morbidity and mortality related to HIV and AIDS. In addition, 88% (n=44) of the participants indicated that by 2022 the country will achieve zero new HIV infection and only 12% (n=6) did not realise the dream of ‘zero new HIV infection by 2022 coming into fruition.
Test and Start for all HIV positive people: The issue of Test and Start being worth providing to “all” HIV positive individuals was supported by almost all the participants (98%, n=49). However, 62% (n=31) of the participants reported that Test and Start was a complicated program and 38% (n=19) indicated it was not a complicated initiative.
Sustainability of test and start: More than half of the participants (68%, n=34) reported that Test and Start was a sustainable initiative while 32% (n=13) reported that Test and Start was not sustainable.
Willingness to provide test and start: A majority of the participants (70%, n=35) indicated that they were comfortable providing Test and Start, whilst slightly above a quarter of them (30%, n=15) were not comfortable providing Test and Start services.
Test and Start Initiative effectiveness: Eighty six percent (86%, n=43) indicated that Test and Start was an effective strategy in the management of HIV. On another note, 56% (n=28) of participants, complained that Test and Start increases the workload and 44% (n=22) indicated that it does not. Moreover, 92% (n=46) of the participants indicated they would want to attend Test and Start training and 8%, (n=4) were not interested on Test and Start training because they were trained.
Attitude level of the participants: The findings indicates that most of the participants (66%, n=33) had poor attitudes towards Test and Start, 28% (n=14) had fair attitude and only 7.3% (n=3) had a good attitude towards the initiative. The participants’ mean score on attitude was 13.3 with a standard deviation of 7.9. In the overall, the participants had a negative attitude.
Objective 3
To determine the association between socio-demographic variables, knowledge and attitude of nurses towards Test and Start Initiative. There was a significant relationship between the age of the participants and the work duration (r=0.927, p=0.001). This means that, the older the participant, the higher the number of years of experience in HIV management settings. For instance, those aged above 40 years were found to have worked 15 years and above in HIV management settings. Training was significantly related to being aware of the Test and Start Initiative (r=0.419, p=0.002), which means that, most of those who were trained had high level of awareness on Test and Start Initiative. Awareness was also associated with comfort in providing Test and Start services (r=0.542, p=0.001). Participants who had high level of awareness on Test and Start Initiative were more comfortable in providing Test and Start services. The data supported a positive relationship between attitudes and comfort in providing Test and Start services to clients (r=0.403, p=0.004) [9-11]. Those who had positive attitudes towards the Test and Start Initiative were more comfortable in providing Test and Start services. Attitudes were related to training on Test and Start Initiative (r=0.349, p=0.013). This explains the fact that participants who had attended training on Test and Start had positive attitudes towards the Initiative. Knowledge was associated with attitudes (r=0.394, p=0.005). This means that those who were knowledgeable about the initiative had positive attitudes towards Test and Start.
Socio-demographics
The findings of this study indicated that the mean age of the participants was 33.8 years. This could perhaps suggest vast experience among the participants as most of them had worked more than five years as evidenced by mean work duration of 8.4 years. This finding is supported by works of [1] who linked experience with knowledge. Nurses who have been working for a long time in HIV management gain expertise thus are more likely to work effectively in HIV initiatives. Consistent with Marranzano et al. [12] participants in the current study were bachelor’s degree holders. Marranzano et al. [12] reported that degree holders showed high levels of knowledge. This finding implies that the higher the qualification, the higher the level of knowledge of individuals. Nurses who are empowered with knowledge become are open minded and critical thinkers who are more likely to have positive attitudes towards newly introduced initiatives including Test and Start [12-20].
Knowledge on test and start
In harmony with Mulenga (2017), only 2% of the participants obtained information about Test and Start from research articles. Mulenga (2017) reported that among the frontline nurses; nursing journals and medical journals were the least consulted sources. This finding is however contrary Mohammed (2016) who reported that slightly above half of the participants indicated that medical textbooks and retraining courses were predominant sources of information on HIV management. The possible meaning of this finding could be that knowledge is not only influenced by the nurse’s personal attributes, but also the organizational factors like lack of information resource centres within facilities. Contrary to Kutoane and Beer (2014), the current study showed that more than half of the study participants were knowledgeable ART first line combination even though they were not trained on Test and Start. In Swaziland exiting students undergo special training, Integrated Management of Adult and Adolescent Illness (IMAI) strategy, which could possible explain why they were knowledgeable on ART. Hence, they were familiar with ART first line combination. Nurses who are knowledgeable about first line drug of choice are most likely to be able to prescribe accordingly. The study findings show that only one-third of the participants had good knowledge on the components of Test and Start initiative. This is consistent with a study by Ouzouni et al. [19] indicating that whilst overall scores confirmed they possessed good knowledge, however demonstrated knowledge deficit on HIV management. A study by Mulaudzi [17] revealed that nurses coped well if they have high level knowledge. This could mean that the efforts in making sure that health providers’ knowledge is at the highest level, are not adequate.
Attitudes towards test and start initiative
Consistent with Kurth et al. [10] the current study showed that most of the participants acknowledged that Test and Start was a preventive initiative. The results emphasize treatment as prevention, because those individuals who are on ART are more likely to have a suppressed viral load and reduced risk of transmitting HIV to partner. Noteworthy, about a quarter of the participants does not support this notion. This could be a barrier in rolling out the Test and Start initiative. Participants in the study also indicated that Test and Start initiative was a complicated programme. In harmony with provision of HIV management was thought to be challenging and costly. This suggests that there may be a need for simplified packages for nurses Above a quarter of the participants indicated that they were not comfortable providing Test and Start services. This is supported by Hassan et al. [6] in a study on Jordan nurses, who reported fear as another factor influencing HIV service delivery. This suggests that some health care workers might be reluctant to provide Test and Start services. Though most of the participants indicated that Test and Start was an effective initiative, more than half of the participants complained that its increased workload. The study supports evidence from Ruud et al. [21] who reported that unhappy health workers were likely to have negative attitudes. These reflect that staff shortage could affect provision of innovative initiatives. The possible result for this could be massive burnout among the staff, with a sluggish progress in rolling out Test and Start. Contrary to expectation that knowledge is a predictor of positive attitudes, the study reported that about two thirds of the participants exhibited negative attitudes towards Test and Start initiative. The results are in support of a study by Gledović, Rakočević, Mugoša, & Grgurević who reported that a high proportion of health care workers showed negative attitude regarding HIV testing. These findings suggest that knowledge is not the sole predictor of attitude, as observed by Iwoi et al. [8] who indicated that good HIV and AIDS knowledge was observed to be the only independent predictor of positive attitude towards HIV care [21-27].
Association between socio-demographics, knowledge and attitudes
Evidence Chan [2] supported that work duration or years of experience were significantly related to both knowledge and attitudes. However, this does not appear to be the case in the current study. The data did not support a relationship between work duration and knowledge as well as attitudes. This finding was contrary to Okpala [20] indicating that those who had worked at least four (4) years had good knowledge. Furthermore, this result is also not consistent with Shabani, who indicated that those who have been providing the service for at least four (4) years were comfortable and happy. This suggests that under normal circumstances with increasing work experience knowledge increased and attitude improves. The findings indicate a significant relationship between training and attitude. This explains the fact that most participants who never attended training on Test and Start had negative attitudes towards the Test and Start Initiative. Consistent with this study, [3] indicated that training improved the attitudes of nurses, however not reaching the desired level. It was reported that a significantly high proportion of trained nurses would refuse to provide HIV services. This suggests that their determinants influencing of attitudes are multifactorial and not only training.
Implications
Although the study has significant findings, it is imperative to acknowledge that there were shortcomings that placed restrictions on the methodology and conclusions. Participants of the study were difficult to get due to staff shortages at their respective departments. On another note 50 participants were targeted, which is a relatively small sample size, hence the findings can be generalized with caution to other settings.
The purpose of the study was to investigate the knowledge and attitude of nurses towards Test and Start in one health facility in the Hhohho Region. A quantitative descriptive cross-sectional study design was employed in this study with a total of fifty participants, selected using simple random sampling. All the participants were registered nurses with at-least one-year work experience in a department providing Test and Start. A structured questionnaire was a tool used to collect the data and a self-administered method of data collection was employed to all the participants. The collected data was analysed using descriptive statistics and Pearson’s correlation. The results of the study show that awareness on Test and Start among participants was high, but knowledge was inadequate, and the participant had poor attitudes towards Test and Start.
For more open access journals in Crimson Publishers, please click on link: https://crimsonpublishers.com/
For more articles in Infectious Disease Open Access Journals, Please click on link: https://crimsonpublishers.com/cjmi/
Disinfection of Mycotic Species Isolated from Cases of Bovine Mastitis Showing Antifungal Resistance by Mary Garvey in Cohesive Journal of Microbiology & Infectious Disease
https://crimsonpublishers.com/cjmi/fulltext/CJMI.000571.php

Fungal disease has emerged as a major medical problem with resistance to the four classes of antifungal agents a common factor promoting fungal virulence. Mycotic infection has a high mortality rate in immunocompromised persons as prolonged aggressive colonisation occurs. As such the medical and veterinary importance of recalcitrant fungal disease is undeniable. Studies described herein detail fungal species associated with bovine mastitis, resistance levels and investigate biocidal control options for use in situ. Effective biocidal options for prophylactic disinfection are suggested to limit fungal transmission with the overall aim of protecting animal health and the food chain.
Keywords: Mycotic; Mastitis; Resistant; Biocidal Efficacy; Protect; Dairy
Bovine mastitis represents a serious and persistent problem for the dairy industry with reduced milk yield, economic costs and often severe consequences for diseased animals. Typically, clinical and subclinical forms are treated with antibiotics as bacterial species are frequently suspected as the causative agent of the intramammary infections (IMIs). Unsuccessful antibiotic therapy, however, leads to continued morbidity and horizontal pathogen transmission within herds with the proliferation of antimicrobial resistance (AMR) an associated issue. Furthermore, persistent non-responsive IMIs often leads to culling of dairy cows in an attempt at curbing disease transmission. Mycotic species are emerging globally as the etiological agents of disease particularly in epizootic hard to treat cases. Fungal infections are hard to recognise, difficult to treat and often chronic in nature. Indeed, the use of antibiotic and corticotherapy which are recommended for IMIs both prophylactically and curatively may lead to mycotic proliferation within the mammary gland [1]. Studies report mycotic IMIs resulting from Candida species colonising the bovine mammary gland, where they are considered opportunistic pathogens having the ability to use antibiotic drugs as nutrient sources, proliferating their growth [2]. Candida albicans, non-Candida albicans species, Trichospron and Cryptococcus neoformans are recognised commensal and environmental pathogens associated with bovine mastitis. Candida and Cryptococcus are important zoonotic species imperative for public health safety as they lead to invasive fungal infections in humans causing serious morbidity and mortality. The elimination of antagonistic bacterial species via antibiotic treatment encourages mycotic reproduction with an influx of immune cells to the udder potentially leading to systemic fungemia. This dysbiosis within the mammary gland may promote clinical symptoms and negatively impact milk quality and yield. Mycotic mastitis resulting from fungal infection is correlated with poor environmental and fomite cleanliness, dirty bedding, contaminated therapy solutions, seasonality and humid temperatures [3]. Fungal virulence factors such as biofilm formation, secretion of aspartyl proteinases, haemolysin production, spore formation and favourable temperature requirements play a significant role in their pathogenicity. Fungal enzymes enable the invasion of tissues from the mammary gland and allows for the development of systemic infections. Mycotoxins, a group of highly toxic compounds produced by fungal species including ochratoxin, zearalenone and fumonisins have been identified in bovine milk [4]. Antifungal drug therapy has been used for mycotic mastitis but there is a lack of evidence relating to drug efficacy and fungal and yeast resistance [3]. As public awareness of food safety increases the recognition of zoonotic pathogens as contributors to global incidence of disease is a key topic of concern. Indeed, as many as half a million people suffer from candidiasis worldwide, with a staggering annual mortality rate of 45-75% [5]. Prophylactically protecting bovine health using adequate environmentally friendly disinfectants is key to safeguarding animal and human health, a key component of “One Health”. An effective prevention and control strategy including udder hygiene, environmental disinfection and milking machine sanitisation is required to reduce and eliminate disease within herds while also protecting the food chain. This study reports on the antifungal resistance of mycotic species isolated from bovine cases of mastitis where animals were non-responsive to antibiotic therapy and subsequently culled. Bacterial isolates from each case which were assessed for susceptibility and resistance to veterinary prescribed antibiotic agents, previously reported by Meade et al. [6] where no resistance to the treatment regime was evident bacterial species. Effective antifungal biocide solutions are also identified for application in animal housing and milking parlour environments. Pathogen dissemination and proliferation can be controlled by proper disinfection of housing areas, milking machines and equipment. Such measures have reduced the risk of bacterial environmental and contagious mastitis and show potential at controlling fungal transmission.
Intramammary infections
The following research presented is in continuation of ongoing studies conducted on various microbial pathogens isolated from dairy cows suffering with chronic cases of IMI post-partum. Previously bacterial species isolated, including S. Uberis, B. cereus, S. aureus, A. buamannii, P. aeruginosa and E. coli, were assessed and reported on [6]. In many cases of chronic mastitis, culling of the animal from the herd is not uncommon, where persistent symptoms often leave farmers no other option. This scenario can be seen in prior cases reported, where patients continued to remain unresponsive to antibiotic treatment. Therefore, further studies on isolated pathogenic fungal species were carried out. In addition to previously reported cases, a further case investigated included a 7-year-old Holstein/British Friesian cross lactating dairy cow presenting with inflamed, chronic mastitis 19 days post-partum. Clinical symptoms of heat, swelling, redness and pain were apparent in two front affected quarters where milk consumption was watery with clots present. Patient initially prescribed IM dexamethasone (2mg/ml) at a dose of 1.5mL per 50kg for 10 days. Dexamethasone was further prescribed 3 weeks later at the same dose, in combination with Tylosin (10mg per kg per day) for 5 days, where IM injection of procaine benzyl penicillin and dihydrostreptomycin (4ml per 100kg bodyweight) had also been used intermittently on two separate occasions for 3 consecutive days at a time to help treat symptoms. Cow remained unresponsive to treatment and was culled from the herd. Microbial analysis identified various pathogenic Gram-negative and Gram-positive species as well as fungal pathogens, Candida krusei and Candida tropicalis, where the total viable count (TVC) was 8.83E+04TVC/mL. Pathogenic species isolated and used for this study were obtained from all reported cases and are as follows Candida albicans, Candida krusei, Candida tropicalis, Cryptococcus neoformans, Trichosporon lactis and Wickerhamomyces anomalous.
Microbial isolation and identification
Collected samples of intramammary infection were inoculated in sabouraud dextrose broth (Cruinn Diagnostics, Dublin, Ireland) and incubated under rotary conditions (125rpm) at varying temperatures of 25 ℃, 30 ℃ and 37 ℃ respectively for up to 72hours, streaking intermittently onto sabouraud dextrose agar (Cruinn Diagnostics, Dublin, Ireland). Fungal total viable cell counts were performed by diluting milk samples in sterile phosphate buffered saline (PBS) with standard plate counts performed after 48-72 hours incubation. Individual colonies were re-streaked for isolation and pure isolated colonies inoculated into sabouraud broth for further biochemical characterization. Colonies were identified based on their morphological characteristics, biochemical profile and growth on selective agars, specifically CHROMagar™ Candida (CHROMagar, Paris) and HiMedia™ Cryptococcus Differential Agar. Identity was confirmed via colony polymerase chain reaction (PCR). Specifically, a single colony of each fungal isolate was picked from a 48-hour culture using a sterile micropipette tip and suspended in 100µl sterile deionized water. Fungal primers ITS1-F 5’-CTT GGT CAT TTA GAG GAA GTA A-3’ and ITS4 5’-TCCTCCGCTTATTGATATGC-3’ (Sigma Aldrich, Dublin, Ireland) were used for direct amplification of intergenic spacer regions (ITS) of rDNA. Direct colony PCR was performed in a total reaction volume of 20µl, containing 17µl red Taq 1.1x master mix (VWR, Dublin, Ireland) 1µl ITS1F, 1µl ITS4 and 1µl of selected colony suspension. DNA amplification was performed in a thermo cycler (VWR, Dublin, Ireland) using the recommended parameters. Clean-up and gene sequencing of PCR products was completed by Source Bioscience (Waterford, Ireland). Strains were stored and cultured in sabouraud broth/agar (at 30 ℃ for Candida spp., Cryptococcus neoformans and Trichosporon lactis, and 25 ℃ for Wickerhamomyces anomalous) and identity confirmed via Gram stain prior to each experimental set up.
Kirby Bauer disk diffusion assay using antifungal drug therapy
Antifungal susceptibility patterns of isolated mastitic strains to amphotericin (Amp B), caspofungin and fluconazole (Sigma Aldrich, Dublin, Ireland) were assessed via disc diffusion method. Three reference control strains, Candida krusei ATCC 14243, Candida albicans ATCC 10231 and Cryptococcus neoformans ATCC 32045 were included for quality control and sensitivity analysis to disease isolates. In addition, the effect of DMSO on fungal growth was evaluated by testing the different concentrations without the antifungal agent to negate the effect of DMSO induced toxicity, as it was used for drug dissolution. The Kirby Bauer assay was conducted as per Meade et al. [7,8] with zones of inhibition measured in millimetre (mm) following 48 hours incubation at 30 oC for Candida spp., C. neoformans and T. lactis, and 72 hours incubation for W. anomalous at 25 oC. Concentrations tested ranged from 2.5 to 50µg/mL for Amp B, 2.5-200µg/mL for caspofungin and 2.5-250µg/mL for fluconazole.
Pasteurisation
Flash pasteurization or high-temperature short-time (HTST) pasteurization is a commonly used standard heat method in which perishable beverages such as milk is subject to high temperature for a short time in order to kill spoilage microorganisms, to allow for extended unrefrigerated storage and to retain flavour. Specifically, the pasteurization process was conducted as per Meade et al. [6], whereby 1mL of microbial suspension containing 1x10⁷cfu/ml was transferred to 9ml sterile full fat milk. The resulting suspensions were then heated to 72 °C for 15 secs followed by rapid cooling to 4 °C. Subsequently, the test solution was 10-fold serially diluted and 500µl aseptically spread on sabouraud dextrose agar plates in triplicate. All plates were inverted and incubated at 30 °C for Candida spp. for 48 hours, 30 °C T. lactis and C. neoformans for 72 hours and a 5-day incubation period at 25 °C for W. anomalous. Surviving colonies were counted and reported as log10 cfu/ml compared to an untreated control. Antifungal resistance was re-assessed after the pasteurization process to determine if heat treatment impacts on the levels of resistance of isolates.
Novel biocidal options
The antimicrobial agents investigated in this study are pure biocides used as disinfectants alone or in commercial brands. The concentrations described are the concentration of the active component and include the concentration used following manufactures instructions. Test solutions studied for use in veterinary areas and as farm disinfectants utilise peracetic acid or triameen as active ingredients. Peracetic acid is a powerful oxidant capable of oxidising the outer cell membranes of micro-organisms, acting as a biocidal disinfectant. Triameen is a fatty amine derivative and a highly effective antimicrobial agent. Studies by Meade et al. [6] have demonstrated the antimicrobial potential of both disinfectants on reference strains sourced from the American Type Culture Collection (ATCC) bank. In the present study, the activity of both biocides will be determined against multidrug resistant fungal pathogens isolated from incidents of mastitis in dairy cows where mortality was the end result in some cases.
Kirby Bauer disk diffusion assay using novel biocidal solutions
The Kirby Bauer assay was carried out on all test isolates to determine the effect of disinfectants on microbial species with the presence and absence of an interfering substance. 1mL of ca. 1x10⁷ microbial cells was added to 9mL BSA to give a working microbial count of 10⁶ cells in solution with 3g/L or 10g/L BSA and with 10g/L yeast extract (YE) (Sigma, Ireland) as low- and high-level interfering substance. Subsequently, 100μL 10⁶ cells/mL microbial suspension were transferred onto replicate agar plates and spread with a sterile L-shaped spreader (Cruinn Diagnostics) to ensure even disruption across the agar surface. Filter disks (6mm) were immersed in the test biocide solutions at concentrations of 0.01,0.1 and 1% (v/v) for 15 seconds and excess solution was al-lowed to drip off the disk. Subsequently, the disk was placed on the inoculated plate. Plates were then incubated for the required time period and temperature. Zones of inhibition were then measured using a Vernier calliper in millimetres as per Meade et al. [7], for each test chemical and each test organism.
Antifungal activity suspension test BSEN 1650
Suspension tests were conducted as per the methods of the European guidelines for fungicidal or yeasticidal testing of chemical disinfectants that form a homogeneous physically stable preparation in hard water for use in in food, industrial, domestic and institutional areas. Isolated strains from the all described cases of mastitis were used for this suspension test. Test Candida species were cultured for 16 hours (C. neoformans and T. lactis required 48-hour culture period while W. anomalous required a 5-day culture period), after which cell counts were adjusted to 107cfu/ml with sterile PBS. Chemical test solutions were prepared as per manufacture instructions for use on site and at a concentration above and below this working concentration giving a range of 0.01,0.1 and 1% (v/v). Prior to testing all reagents are equilibrated to the test temperature of 20 °C using a water bath. Subsequently 8 ml of the test product was transferred to a sterile container with 1ml of sterile water. Afterward, 1ml of microbial suspension containing 1x107 fungal cells was added. Additionally, 1ml of interfering substance at 3.0g/L BSA (low level soiling) and 10g/L BSA with 10g/L YE (high level soiling) was added with subsequent incubation for 0 to 15 minutes with mixing in a 20 °C water bath. At set intervals of 5,10 and 15 minutes 1ml of the test mixture was transferred into a tube containing 8ml neutralizer and 1ml of sterile water. Samples were mixed and incubated in the water bath for 5 minutes. After neutralization with 30g/l polysorbate 80+3g/l lecithin/l-a-phosphatidylcholine from egg yolk (Sigma, Ireland), 100µl of this bacterial suspension was transferred onto agar plates in triplicate and incubated at 30 °C for 48 hours for Candida spp, 30 °C for 72 hours for C. neoformans and T. lactis and a 5 day incubation period for W. anomalous at 25 °C. Surviving cells of treated organisms was counted to determine the level of fungal inactivation following exposure to the test solutions compared to the untreated control (PBS). For compliance with this test, test chemicals must achieve a 104 fungal cell reduction in treatment times less than 30 minutes.
Statistics
All the experiments were performed three times with three plate replicates for each experimental data point providing a mean result for each experimental batch. Average zone diameter was calculated for the Kirby Bauer assay with standard deviation and significance levels at 95% confidence determined for each strain. For suspension testing the log10 reduction was calculated as the log reduction in viable cell numbers (cfu/ml) of the non-treated (N0) and treated (N) samples [log10 (N0/N)]. Student T tests were conducted to determine significance levels (p<0.05) of fungal susceptibility to treatment and levels of susceptibility or resistance between species investigated using Minitab 16 (Minitab Ltd, Coventry, UK).
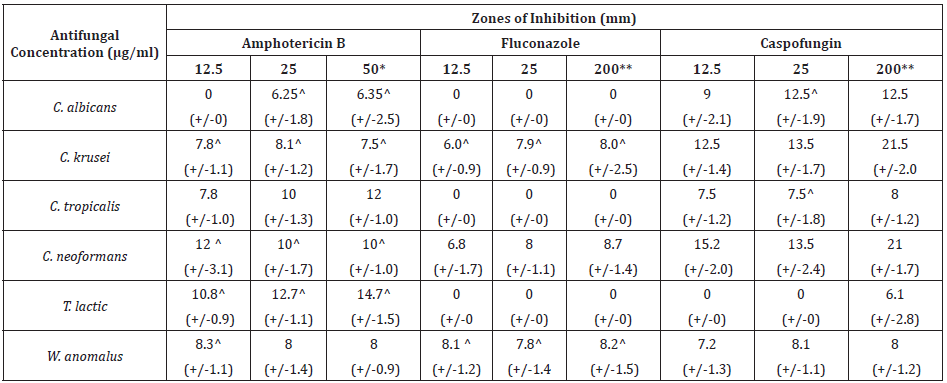
Table 1 shows antifungal susceptibility of isolated species Candida albicans, Candida krusei, Candida tropicalis, Cryptococcus neoformans, Trichosporon lactis and Wickerhamomyces anomalus to antifungal therapeutic agents. Amphotericin B provided zones of inhibition for all strains with the most sensitive strain being T. lactic followed by C. tropicalis, C. neoformans, W. anomalus, C. krusei and C. albicans at 50µg/ml. At concentrations exceeding this no increase in zone diameter was achieved for Amphotericin B. Quality control ATTC strains of C. albicans, C. krusei and C. neoformans proved more sensitive to Amp B than their isolated counterparts at 50µg/ml. Where a zone diameter of 14,8 and 15mm was obtained for C. albicans (ATCC 19231), C. krusei (ATCC 14243) and C. neoformans (ATCC 10231) (data not shown) compared to 6.3,7 and 10mm for the isolated counterparts (Table 1). C. albicans, C. tropicalis and T. lactic demonstrate clear resistance to fluconazole at concentrations of up to 200µg/ml. C. neoformans displayed the greatest sensitivity (8.7mm) to fluconazole followed by C. krusei and W. anomalus with optimal inhibition at 200µg/ml. Fluconazole provided zones of inhibition of 0,7 and 18mm for control strains of C. albicans (ATCC 10231) and C. krusei (ATCC 14243) and C. neoformans (ATCC 32045) respectively, demonstrating drug efficacy for non-isolated species (data not shown) with the exception of C. albicans ATCC. T. lactic displayed resistance to caspofungin up to 200µg/ml with this concentration giving a zone diameter of 6.1mm only. All other test isolates show sensitivity to caspofungin with optimal inhibition obtained at 200µg/ml, where a zone diameter of 21.5,21,12.5,8,8 and 6.1mm was obtained for C. krusei, C. neoformans, C. albicans, C. tropicalis, W. anomalus and T. lactic respectively. A diameter of 20,21 and 5mm was obtained for 200µg/ml caspofungin on control ATCC strains of C. albicans, C. krusei and C. neoformans respectively suggesting increased sensitivity in isolated species. As with fluconazole concentrations exceeding 200µg/ml did not provide an increase in zone diameter for any strain tested.
Table 1: Zones of inhibition (mm) produced by licensed antifungal agents against zoonotic fungal isolates from mastitis cases in dairy (+/- Standard deviation).
*No increase in zone diameter was achieved with concentrations of AMP B exceeding 50μg/ml. **No increase in zone diameter was achieved with concentrations of fluconazole and caspofungin exceeding 200μg/ml. ^indicates test species which showed statistically significant decreased zones of diameter post-pasteurisation compared to pre-pasteurisation
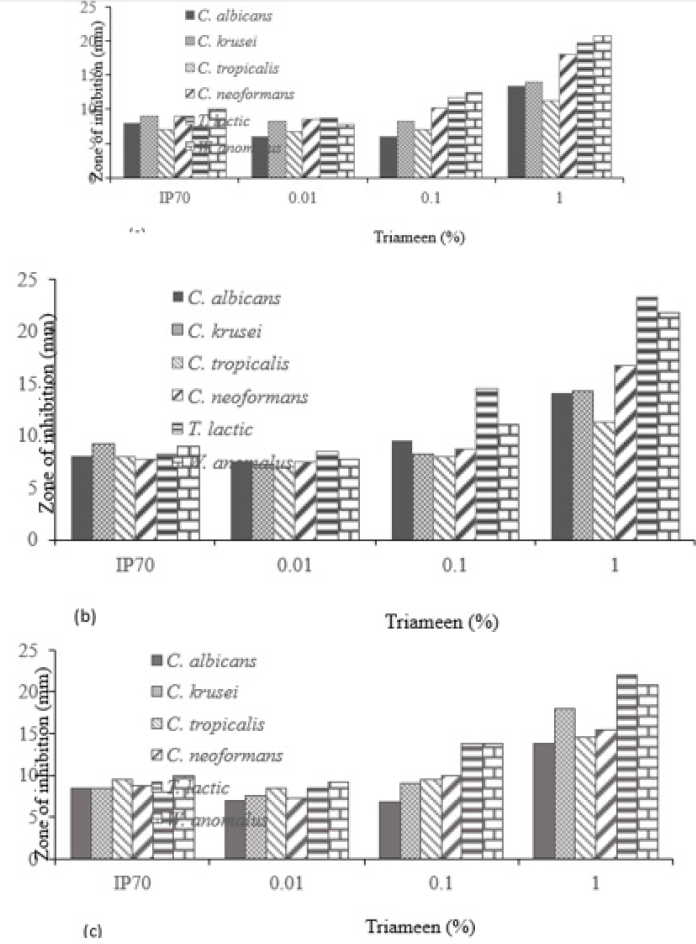
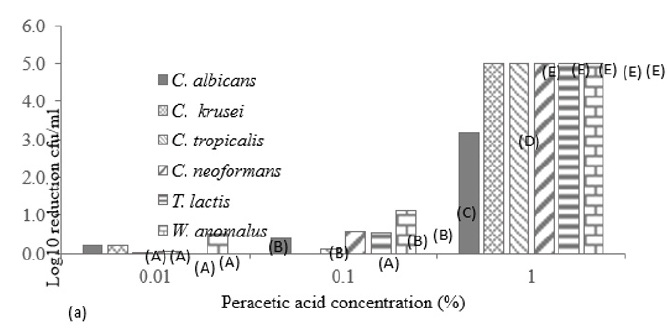
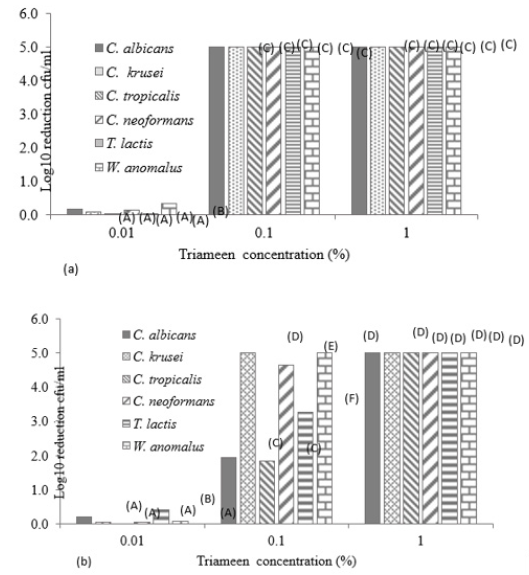
Figure 1 displays the viable and non-viable cell numbers of all test isolates pre and post flash pasteurisation. For all test species, significantly high numbers remained viable post treatment with the order of decreasing survivability as follows: T. lactic, W. anomalus, C. krusei, C. tropicalis, C. albicans and C. neoformans. C. neoformans proved most sensitive to flash pasteurisation with a 3.3 log10cfu/ml death of treated cells compared to the 1.5 log10cfu/ml death achieved for T. lactic. Interestingly, an increase in resistance to Amp B was observed in T. lactic following pasteurisation (Table 1) evident as decreased zone diameters. A zone diameter of 14.7mm pre pasteurisation and 4.75mm post pasteurisation for T. lactic was obtained at 50µg/ml Amp B. This post heat treatment increase in resistance to Amp B was also observed for C. albicans, C. krusei and C. neoformans (complete resistance emerged). C. krusei and W. anomalus also demonstrated increased resistance to fluconazole post flash pasteurisation. This constitutes an important find as all fungal isolates show clear resistance to heat treatment with increased antifungal resistance also present in certain treated species. All isolated strains demonstrate susceptibility to peracetic acid at 1% with zones exceeding that of the control chemical 70% iso propyl alcohol with and without the interfering agent BSA (Figure 2). At all concentrations of peracetic acid, W. anomalus proved consistently the most sensitive strain tested with a zone of inhibition of 40mm for all concentrations of BSA. This reduced to ca. 23mm at 0.1% peracetic acid for this strain. C. albicans proved the most resistant strain with zones of inhibition of ca. 18mm followed by C. tropicalis. IP70% provided consistent zones not exceeding 8mm for all species regardless of the presence of BSA. The lowest concentration of peracetic acid (0.01%) provided similar fungal inhibition to the IP70% for C. krusei, C. tropicalis, T. lactic and W. anomalus (Figure 2a) in the absence of BSA with no inhibition of C. albicans evident. The presence of the interfering substance BSA at 3 and 10g/L does appear to affect the effectiveness of peracetic acid at 0.01% but not at concentrations exceeding this. Compared to peracetic acid, triameen demonstrated less efficacy at inhibiting fungal growth for all species (Figure 3) with T. lactic the most sensitive strain at 1% concentration. C. tropicalis proved the most resistant strain followed by C. albicans. As with peracetic acid, 0.01% triameen provided similar levels of inhibition to IPA70% irrespective of the presence of BSA. C. albicans did not display resistance to triameen at this lower concentration as observed with peracetic acid. While triameen appears less effective than peracetic acid (demonstrated by reduced zones of inhibition) it appears more effective at the lower concentrations tested and is not inhibited by the presence of the interfering substance. Comparative ATCC strains of C. albicans, C. krusei and C. neoformans proved significantly more sensitive to both biocidal options in the absence and presence of interfering substance. At the highest concentration of 1% peracetic acid in high level soiling conditions a zone of inhibition of 25,24 and 30mm was obtained, with 17.5, 23.5 and 30mm obtained for 1% triameen for ATCC C. albicans, C. krusei and C. neoformans respectively (data not shown). Figure 4 displays the BSEN 1650 biocidal testing of all isolates for peracetic acid where only the 1% concentration provided the necessary 4 log10cfu/ml loss of viability for test strains in both 3 and 10g/L interfering agent in 15 minutes. C. albicans again appears the most resistant to peracetic acid where a maximal 3.2 log10cfu/ml inactivation was obtained at the highest concentration tested of 1% in 15 minutes increasing to the required 4 log10cfu/ml at 30 minutes (data not shown). Triameen appears more effective in this assay with a 4 log10cfu/ml loss in viability of all test strains obtained for 0.1% in the presence of 3g/L BSA in 15 minutes (Figure 5a). A decrease in this effectiveness was observed at the higher concentration of BSA for C. albicans, C. tropicalis and C. neoformans (Figure 5b) suggesting that the presence of organic matter may impede its biocidal efficacy for these strains. Peracetic acid is potent enough to provide the 4log10cfu/ml loss in viability at 1% concentration in both low level (3g/L BSA) and high-level soiling (10g/L BSA and YE) in under 15 minutes. Triameen at 0.1% is potent enough to meet the BSEN requirements in low level soiling environments at 0.1 and at 1% in 15 minutes with 30 minutes needed in high level soiling environments at these concentrations.
Figure 1: Viable and non-viable cell numbers (log10 cfu/ml) (+/- S.D) of zoonotic fungal isolated species post flash pasteurisation of 6 log10 cfu/ml viable cells at 72 ℃ for 15 seconds with rapid cooling to 4 ℃. A, B,C,D,E,F,G and H denotes significant difference at p>0.05.
Figure 2: Zones of inhibition (mm) of peracetic acid and 70% IP for mastitis isolated fungal species (a) in the absence of BSA, (b) presence of 3g/L BSA and (c) 10g/L BSA with 10g/L yeast extract (+/-S.D.).
Figure 3: Zones of inhibition (mm) of triameen and 70% IP for mastitis isolated fungal species (a) in the absence of BSA, (b) presence of 3g/L BSA and (c) 10g/L BSA with 10g/L yeast extract (+/-S.D.).
Figure 4: Log10 reduction in cell viability (cfu/ml) of mastitis isolated fungal species following exposure to varying concentrations of peracetic acid in the presence of interfering agent a) 3g/L BSA and b) 10g/L BSA and 10g/L yeast extract in accordance with BSEN 1650. Data obtained for 15 minutes treatment time (+/- S.D).
Figure 5: Log10 reduction in cell viability (cfu/ml) of mastitis isolated fungal species following exposure to varying concentrations of triameen in the presence of interfering agent a) 3g/L BSA and b) 10g/L BSA and 10g/L yeast extract in accordance with BSEN 1650. Data obtained for 15 minutes treatment time (+/- S.D). A,B,C,D,E and F denotes significant difference at p>0.05.
Go to
Bovine mastitis remains and ongoing problem globally with economical costs and yield losses at production level and animal mortality at herd level. Small dairy holders are particularly impacted by the financial costs of culling animals. Morbidity is more frequent in chronic cases of mycotic mastitis than acute with the excessive use of antibiotics, steroids and immune suppressing drugs contributing factors for mycotic disease. There are 3 categories of risk factors associated with mycosis:1) factors promoting fungal colonization 2) factors suppressing the host immune response and 3) factors that provide a direct route for fungal invasion and infection. Additionally, antibiotic therapy induces a disturbance in udder homeostasis and inhibits neutrophils and T lymphocyte activity, ultimately leading to fungal cell proliferation within the host. Indeed, all cases assessed in this study were fatal cases on IMIs, with susceptibility to antibiotics demonstrated in pathogenic bacterial isolates [6]. Further microbial analysis identified fungal species with clear antifungal resistance present for certain antifungal agents. The etiological agents of mycotic mastitis in this study included Candida albicans, non- albicans Candida (NCAC), Cryptococcus neoformans, Trichosporon lactis and Wickerhamomyces anomalus. Amphotericin B is a fungicidal antifungal drug commonly used for the treatment of Candida mycosis exhibiting effect by binding to cellular ergosterol. Amp B, therefore, induces cell death by creating pores in the fungal cell membrane and the accumulation of reactive oxygen species (ROS) leading to cell damage, apoptosis and death [9]. All isolated species studied demonstrated susceptibility to Amp B with T. lactic the most susceptible species. Trichosporon is a medically important genus associated with gastrointestinal, respiratory tract, skin, and vaginal infections in humans. As an environmental pathogen T. lactic can cause invasive trichosporonosis once entry to the host has been achieved. Amp B binds to ergosterol and to cholesterol (a key component of mammalian cell membranes) with lower affinity, hindering its therapeutic use. Toxicity associated with Amp B includes kidney (renal) cell membrane damage, modulation of intracellular trafficking and eliminating the pH gradient between the endosomes/vacuole and the cytosol [10]. C. albicans, C. tropicalis and T. lactis possessed resistance to fluconazole and low susceptibility to amphotericin B and caspofungin. Indeed, all other isolated species show low levels of susceptibility to fluconazole up to 200µg/ml with zones of inhibition not exceeding 8.7mm. Resistance to azoles is commonly reported in Candida species and is related to alterations in the target enzyme 14α-lanosterol demethylase (14-DM), which is responsible for the production of an ergosterol precursor, encoded by the ERG11 gene. Ergosterol is essential for the fungal cell membrane therefore this inhibition has a fungistatic effect arresting cell growth. Efflux pumps are also associated with Candida resistance due to the CDR1, CDR2 and MDR1 genes [2]. Fluconazole is frequently prescribed for Candida infections in humans resultant from the 5 most common species associated with disease i.e. Candida albicans, Candida glabrata, Candida parapsilosis, Candida tropicalis and Candida krusei [11] all of which are zoonotic in nature. As it emerges that cases of candidemia in animal and humans are frequently resultant from NCAC species it is now essential to establish the level of antifungal resistance in these species. Additionally, Cryptococcus neoformans is an important pathogen frequently associated with pulmonary cryptococcosis and cryptococcal meningitis in immunocompromised persons having impaired cell-mediated immunity. The echinocandin caspofungin proved the most effective antifungal used as the greatest inhibition was evident, except for T. lactic which proved quite resistant, at 25µg/ml. C. tropicalis also appears more sensitive to Amp B than the other antifungal agents. Both important zoonotic species C. neoformans and C. krusei displayed susceptibility to all antifungal agents tested in the following order of decreasing sensitivity: caspofungin, Amp B and lastly fluconazole. A similar pattern emerged for W. anomalus. Echinocandin drugs are the favoured therapeutic for the treatment of candidiasis having effect by inhibiting the biosynthesis of critical glucan polymers in fungal cell walls. Echinocandin resistance in susceptible species, however, is emerging and is typically acquired during therapy [12]. The mechanism of caspofungin resistance is due to amino acid alterations in glucan synthase, decreasing the sensitivity of this enzyme to the antifungal. The echinocandins have the added benefit of an excellent therapeutic index with low mammalian renal and hepatic toxicity or severe drug-drug interactions making them a safer antifungal option. Pasteurisation remains the method of choice for the processing of milk pre-consumption to ensure consumer safety. Previous studies reported by this research group demonstrated the thermal resistance of pathogenic bacterial isolates associated with bovine mastitis [6]. Similarly, HTST pasteurisation of mycotic species demonstrates their resistance to thermal inactivation with all isolated species surviving treatment. T. lactic proved the most resistant with 4.5 log10cfu/ml remaining viable following HTST pasteurisation followed by W. anomalus (4 log10cfu/ml), C. krusei (3.7 log10cfu/ml), C. tropicalis (3.7 log10cfu/ml), C. albicans (3.2 log10cfu/ml), and lastly C. neoformans (2.7 log10cfu/ml). importantly, there was an increase in antifungal resistance seen in C. albicans, C. krusei, C. neoformans and T. lactic post heat treatment indicating that sublethal thermal processing proliferates antifungal resistance to Amp B. This may relate to the presence of heat shock proteins (HSPs) in these species being activated following sublethal exposure. Indeed, studies report the role of HSPs in the proliferation, drug resistance, virulence and biofilm formation of C. albicans [13] and C. neoformans [14]. This is an important find as thermal processing of dairy products at these parameters appears ineffective at protecting the food chain. Invasive fungal infections (IFIs) resultant from contaminated food consumption can cause devastating illnesses and considerable mortality, however, quantifying their public health burden remains challenging [15]. Consequently, the true risk and rate of foodborne IFIs are unidentified. The manifestations and outcomes of foodborne IFIs relate to the fungus and host factors, where immunocompromised persons are particularly at risk. Controlling fungal food spoilage and preventing post consumption pathogenesis is a major issue for food industries where there is an urgent need for efficient solutions to prevent fungal transmission and food contamination in dairy products. Both biocidal options investigated provided excellent antifungal activity with the lowest concentration of each displaying similar activity to the standard IP70%. Additionally, biocidal chemicals peracetic acid and triameen show potential to act as intermediate level disinfectants according to European testing requirements (BSEN 1650). Preventing microbial transmission at all stages of post-harvest, harvest and pre-harvest using effective biocidal solutions is vital to ensure food safety. Effective disinfection of animal housing facilities, milking equipment and milk bulk tanks remains the best prophylactic means of protecting animal health, the food chain and consequently, human health, a key goal of the “One health” initiative.
Antifungal resistance is an ongoing issue, particularly as fungal infections are recognised as a major health problem causing approximately 300 million infections globally with 1.35 million deaths annually. With the increasing awareness that mycotic species are often associated with pathogenesis in both animal and human hosts, there is an immediate need to determine the levels of drug resistance in fungal and yeast zoonotic species. A better understanding of drug resistance including resistance mechanism, cellular and clinical factors promoting resistance and novel methods of overcoming resistance will promote more effective strategies for protecting animal health, the food chain and subsequently, human health. Furthermore, with the environmental impact of climate warming an increase in the incidence of fungal disease is likely to emerge, globally. Findings reported herein detail fungal resistance to Amp B, fluconazole and caspofungin in zoonotic fungal species associated from bovine mastitis where animal culling was conducted to prevent disease transmission. Biocidal options peracetic acid and triameen demonstrate effective antifungal activity in line with the testing requirements of European testing standard (EN1650).
For more open access journals in Crimson Publishers, please click on link: https://crimsonpublishers.com/
For more articles in Infectious Disease Open Access Journals, Please click on link: https://crimsonpublishers.com/cjmi/
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}